When you look at a lesion you are seeking out colours and structures.
Colours in the skin are due to melanin pigment, blood, keratin and collagen and pigments added from the environment. Melanin can be in nevus cells or melanocytes and keratinocytes in the epidermis and also in macrophages and other tumour proliferating cells in the dermis. Melanin is black if very superficial in the epidermis, brown at the dermo epidermal junction , grey in macrophages in the papillary dermis and blue in the deeper nevus cells of a blue nevus or a melanoma metastasis or a pigmented basal cell carcinoma.
Hemangiomas are red or purple while Seb ks are brown, yellow or black if they have a lot of melanin in them.
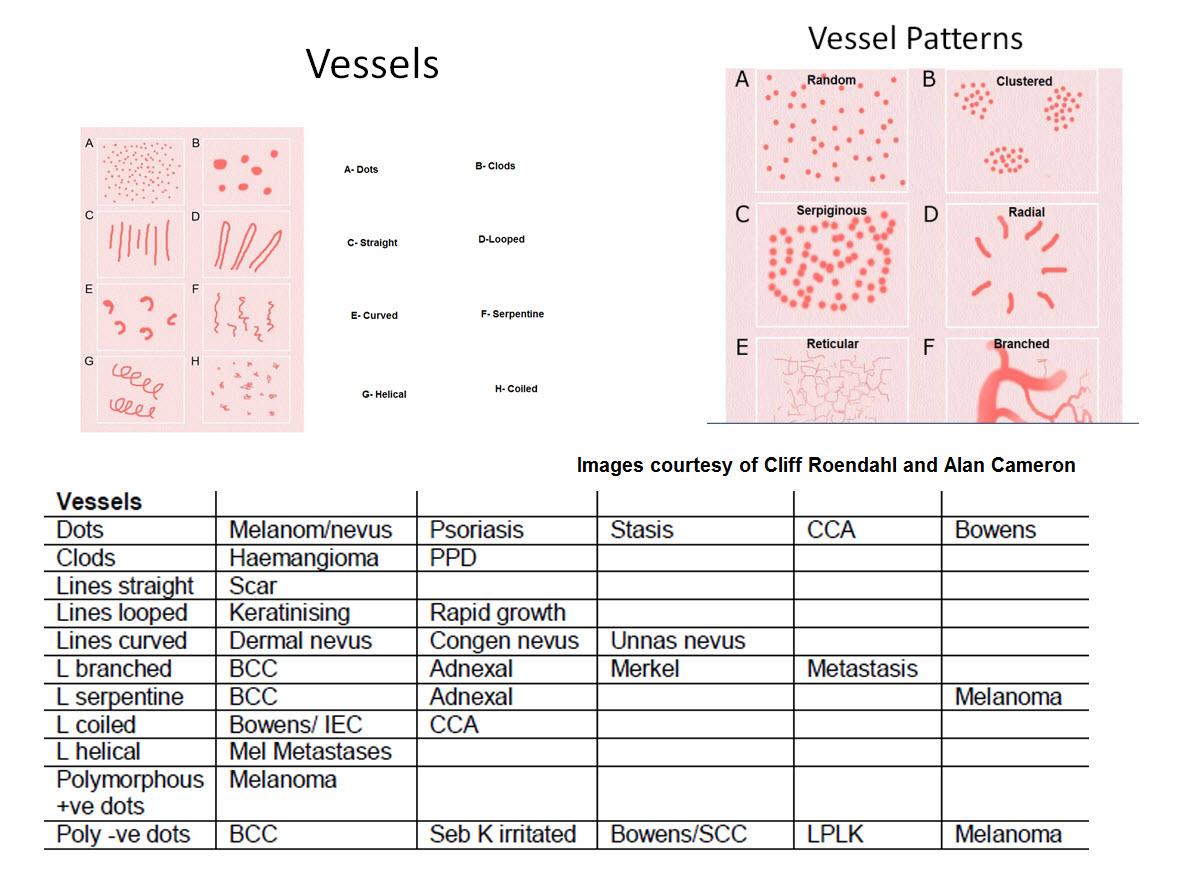
What about structures? Look for lines, circles, dots, clods or one colour structureless areas. With pink lesions you look at the vessels and background white lines to try to make a diagnosis .
Just look at the links opposite for each of these elements and what they represent. Start with Lines and work your way down. If a particular diagnosis is mentioned that you are unfamiliar with then scroll down the links opposite and look it up. This way you will learn what each of the colours and structures might represent and that should help you to make the correct diagnosis. However remember the real question here is not the correct diagnosis but instead do I leave this lesion, cut it out or monitor it over say 3 months. Let me quickly add you do not monitor something that is raised and rapidly growing. You cut it out.
Using a dermatoscope allows you to quickly determine if a lesion is benign. If a pigmented lesion is one colour and symmetrical then ignore it. Move on to the next lesion. I am assuming you can recognise a typical seborrhoeic keratosis and hemangioma. If not look first at the Seb k and hemangioma links opposite and learn the patterns. If it is pink look at the vessels.
Look at the table below to see which lesions commonly have which structures and the patterns in which these structures are arranged. Keep in mind that a symmetrical arrangement of structures is usually a benign lesion. You should also learn all the clues to melanoma. I have added them below but look at the link opposite to see good clinical examples.
Take particular care of lesions that the patient says are new or have changed. Look at them particularly carefully. Know your patient's past history. If they already have had two melanomas then you excise any new pigmented lesion that is not obviously benign.
Take care with new rapidly growing pink papules. They usually all end up needing excised. See Amelanotic Melanoma
So pick up your dermatoscope and let us get started